How To Write A Letter Of Medical Necessity For A Wheelchair
Considerations for medically necessity of common options and accessories include the following. To Whom It May Concern.
Letter Of Medical Necessity 1 Wheelchair Chair

We cant assume that our funding source is going to approve something just because the client has tetraplegia or paraplegia.
How to write a letter of medical necessity for a wheelchair. It suggests that youve established a relationship with the client and the equipment youre. These design templates provide exceptional instances of exactly how to structure such a letter and also include example content to work as a guide to format. Answer We need to document the evaluation of the clients systems including both neurologic and orthopedic their postural assessment and their level of function.
Full name Insurance group number Date of birth Case ID number if available Insurance ID number 2. -Permobil C300 front wheel drive power wheelchair set up for multiple power seat functions to give her safe and independent mobility and access to all areas of her home and her ADLs. Motorized and customized wheelchairs and certain other durable.
A Letter of Medical Necessity LMN is exactly what it sounds like a letter written by your physician andor therapist stating why it is necessary for your child to have the medical equipment you are applying for. As a result of post-surgical complications and prolonged pain _____ has not walked in over. This booklet is a guide to your UT SELECT medical UT SELECT benefits.
Use the clients name whenever possible versus the generic use of client child or patient. First make sure the letter is individualized. When composing a letter of medical necessity LMN for a wheelchair or scooter it is imperative to include the following key phrases within the document in addition to the standard structure and components of the LMN as noted in a previous document as funding sources will seek out this information during the approval process.
Have your physician provide a letter of medical necessity and any. This wheelchair base can accept the power seating functions that she needs to manage her quadriplegia -Flat-free inserts in tires as she cannot fill air tires. We have to state the obvious.
Am writing on behalf of my patient patient name to document the medical necessity of treatmentmedicationequipment item in question for the treatment of specific diagnosisThis letter provides information about the patients medical history and diagnosis and a statement summarizing my treatment rationale. Writing a letter of Medical Necessity for Durable Medical equipment Guidelines applicable to all funding sources and systems Written to obtain approval from third party payers for the purchase of assistive technology a successful letter of medical necessity includes the following features. This helps the reviewer picture this individual as a person and not just a file.
MMDDYYYY Letter of Medical Necessity RE. Using a wheelchair will improve the patients participation in MRADLs. To Whom It May Concern I am writing this letter with regard to _____ and the purchase of an Up n Free Gait Trainer.
If you are submitting for a loan or grant or public service make sure the family has provided authoriza. Health plan requirements may vary so the prescriber should refer to the prior authorization or coverage information specific to their patients health plan before completing a Letter of Medical Necessity. The MRADLs cannot be resolved by using a cane or walker.
The elevating seat allows CLIENT. It also lends the letter a greater sense of authenticity when compared to a generic template. I am writing to request that you please provide funding for a special needs Adaptive Car Seat for Childs name.
Significant extensor tone thus limiting the clients capability to be positioned in a standard seated position. Collection of letter of medical necessity for wheelchair template that will completely match your requirements. The patient will be able to use the wheelchair.
The letter of medical necessity should be written by a medical professional familiar with the requesting partys medical condition. _____ is a ____ year old young woman whose complex medical and surgical conditions as well as her orthopedic and neurological deficits render her completely dependent in mobility. Unfortunately medical providers often only provide the diagnosis and miss other important contextual information about the.
Reader that the requested assistive technology is necessary to meet the medical needs of the person for whom the assistive technology is being requested. Recommended information for a Letter of Medical Necessity includes. Independent transfers in and out of the wheelchair is a medical necessity for individuals of all ages.
Use of this letter does not guarantee coverage for the product. MRADLs are significantly impaired for the patient. I am writing to provide additional information to support my claim for patients name s treatment of osteoporosis with FORTEO teriparatide rDNA origin 20mcg daily injection.
COMPOSING A LETTER OF MEDICAL NECESSITY To whom it may concern. The severity of the patients condition. What needs to be included in a letter of medical necessity for a wheelchair.
Childs first name is a ____year old malefemale with diagnosis of _____ and. The letter should contain more than your childs diagnosis. Documenting medical necessity can seem daunting at times and can vary depending on the type of wheelchair.
A summary of the patients previous treatments the duration of each and. The prescriber should refer to the. 5000 bariatric surgery deductible plan pays 100 of covered servicesfor.
The professional should briefly. In addition to improving independence the seat to floor feature also promotes safety by reducing handling by unqualified people and lowering the level of transfer. Medical documentation for wheelchairs must include the following.
Reclining back or tilt systems may be considered medically necessary if the patient resides within the wheelchair for a minimum of 2 hours per day and has at least one of the following diagnoses. The letter must be written in a formal and. This fact sheet is intended as a guide to preparing such a letter of medical necessity.
Identify the mobility limitation. When composing a formal or business letter presentation design and also style is crucial making a good initial impression. In order to explain the medical condition to the third party the formal medical necessity letter must be written to them.
The patients diagnosis and the indication for the Genentech medicine being prescribed. SAMPLE Letter of Medical Necessity that outlines the information a payer may request. Example Letter of Medical Necessity Restraint System Date.
Https Www Inspiredbydrive Com Wp Content Uploads 2016 12 Toileting Support Lmn Sample Pdf
Free 20 Medical Necessity Letter Templates In Pdf Ms Word Free Premium Templates
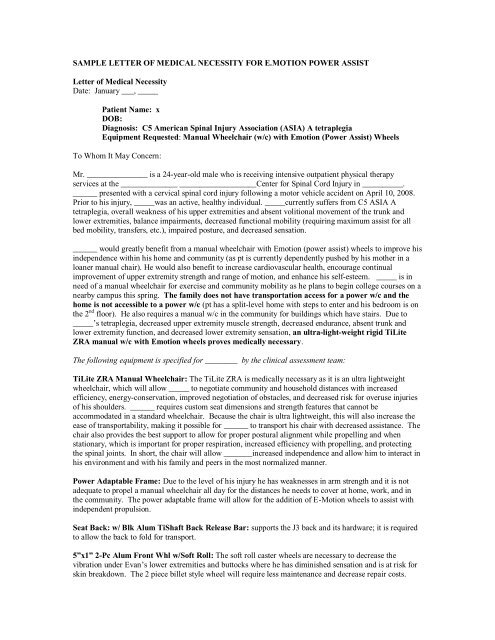
Sample Letter Of Medical Necessity For E Motion
Ot 620 Letter Of Medical Neccessity Anatomical Terms Of Motion Wheelchair


Free 20 Medical Necessity Letter Templates In Pdf Ms Word Free Premium Templates

Sample Letter Of Medical Necessity For E Motion
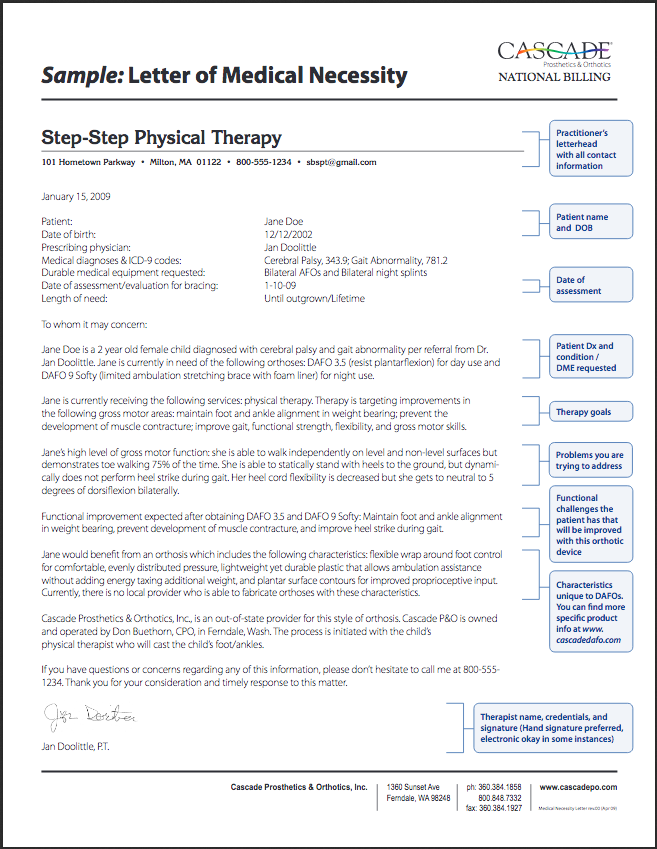
Letter Of Medical Necessity Cascade National Billing
Free 20 Medical Necessity Letter Templates In Pdf Ms Word Free Premium Templates
Https Ngsmedicare Com Ngs Wcm Connect Ngsmedicare 28d08df5 4a3a 43a1 A76f 7132abd9b11b 1592 0614 Dearphysicianletter Manual Wheelchairs Coverage Documentation Pdf Mod Ajperes Cvid Kbyfxtp
Http Levousa Com Wp Content Uploads 2008 12 001 Levo Letter Of Medical Necessity 111207 Pdf
Https Www Convaid Com Wp Content Uploads 2020 06 Handout Writing A Successful Letter Of Medical Necessity Pdf

Letter Of Medical Necessity Orthotics Fill Online Printable Fillable Blank Pdffiller

Insurance Battle Power Wheelchair By Max Gravenstein Hubabl Medium
Free 20 Medical Necessity Letter Templates In Pdf Ms Word Free Premium Templates
Https Www Convaid Com Wp Content Uploads 2020 06 Handout Writing A Successful Letter Of Medical Necessity Pdf

Sample Letter Of Medical Necessity Frank Mobility Sample Letter Of Medical Necessity Frank Mobility Pdf Pdf4pro
Https Www Seatingdynamics Com Wp Content Uploads 2019 02 Seating Dynamics Sample Lmn Breakage Movement 2019 Pdf

Sample Letter Of Medical Necessity For Dental Treatment Trinity Medical Center

Insurance Battle Power Wheelchair By Max Gravenstein Hubabl Medium
Posting Komentar untuk "How To Write A Letter Of Medical Necessity For A Wheelchair"